Managing the revenue cycle for electroconvulsive therapy requires clinical precision and strict adherence to coding guidelines. Behavioral health facilities frequently encounter rejected claims due to minor documentation discrepancies. Understanding the real truth about coding and billing for mental health services means recognizing that specialized psychiatric procedures are heavily audited by Medicare and commercial payers.
This guide provides an objective breakdown of the reimbursement rules surrounding the cpt code for ect, proper documentation standards, and actionable strategies to maintain a compliant and efficient billing cycle.
1. Common Billing Discrepancies: The Anesthesia Crosswalk
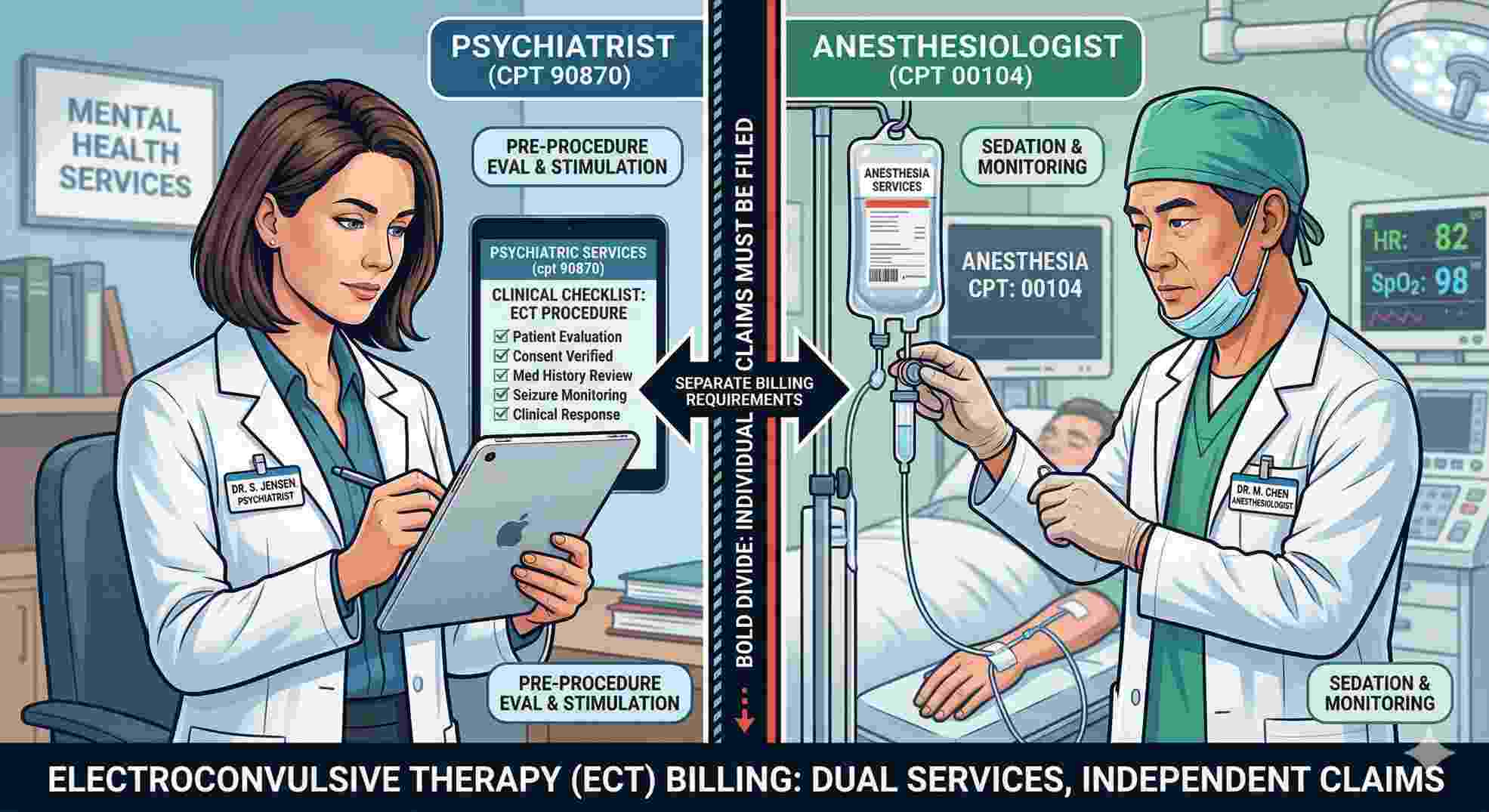
A frequent billing error occurs when practices misunderstand the scope of the primary psychiatric procedure code. CPT 90870 specifically covers the professional psychiatric service—the application of the stimulus and immediate clinical monitoring. It does not cover the administration of anesthesia.
To ensure compliance, the attending anesthesiologist must separately bill their specific code (CPT 00104). Separating the psychiatric professional fee from the anesthesia fee is a critical step in standardizing your revenue cycle and avoiding immediate clearinghouse rejections.
2. Scope and Application of CPT 90870
The American Medical Association (AMA) defines CPT 90870 as “Electroconvulsive therapy (includes necessary monitoring).” In practice, this requires that a credentialed psychiatrist evaluate the patient prior to the procedure, administer the treatment, and manage the immediate clinical response.
Medical coders must view ECT procedure codes as one component of a larger facility encounter. Proper allocation of services prevents bundled claim denials.
| Service Component | Included in CPT 90870? | Billed Separately? | Responsible Party |
|---|---|---|---|
| Application of electrical stimulus | Yes | No | Attending Psychiatrist |
| Immediate post-seizure monitoring | Yes | No | Attending Psychiatrist |
| Full Evaluation and Management (E/M) | No | Yes (Requires Modifier 25) | Attending Psychiatrist |
| Intravenous general anesthesia | No | Yes (Use CPT 00104) | Anesthesiologist |
| Surgical suite or recovery room fee | No | Yes (Via Revenue Codes) | Hospital or Surgery Center |
| Routine intra-procedure EEG | Yes | No | Attending Psychiatrist |
3. Aligning Clinical Documentation with Procedure Codes
Medical auditors require specific, undeniable proof that the treatment aligns with the billed codes. Clinical documentation must flawlessly match the requirements of the procedure.
The provider’s note must explicitly clear the patient for the procedure on the date of service. Furthermore, the electronic health record (EHR) must capture exact numeric data, including the duration of the electrical stimulus, the exact length of the motor seizure, the length of the EEG seizure, and the specific electrode placement (unilateral, bilateral, or bifrontal).
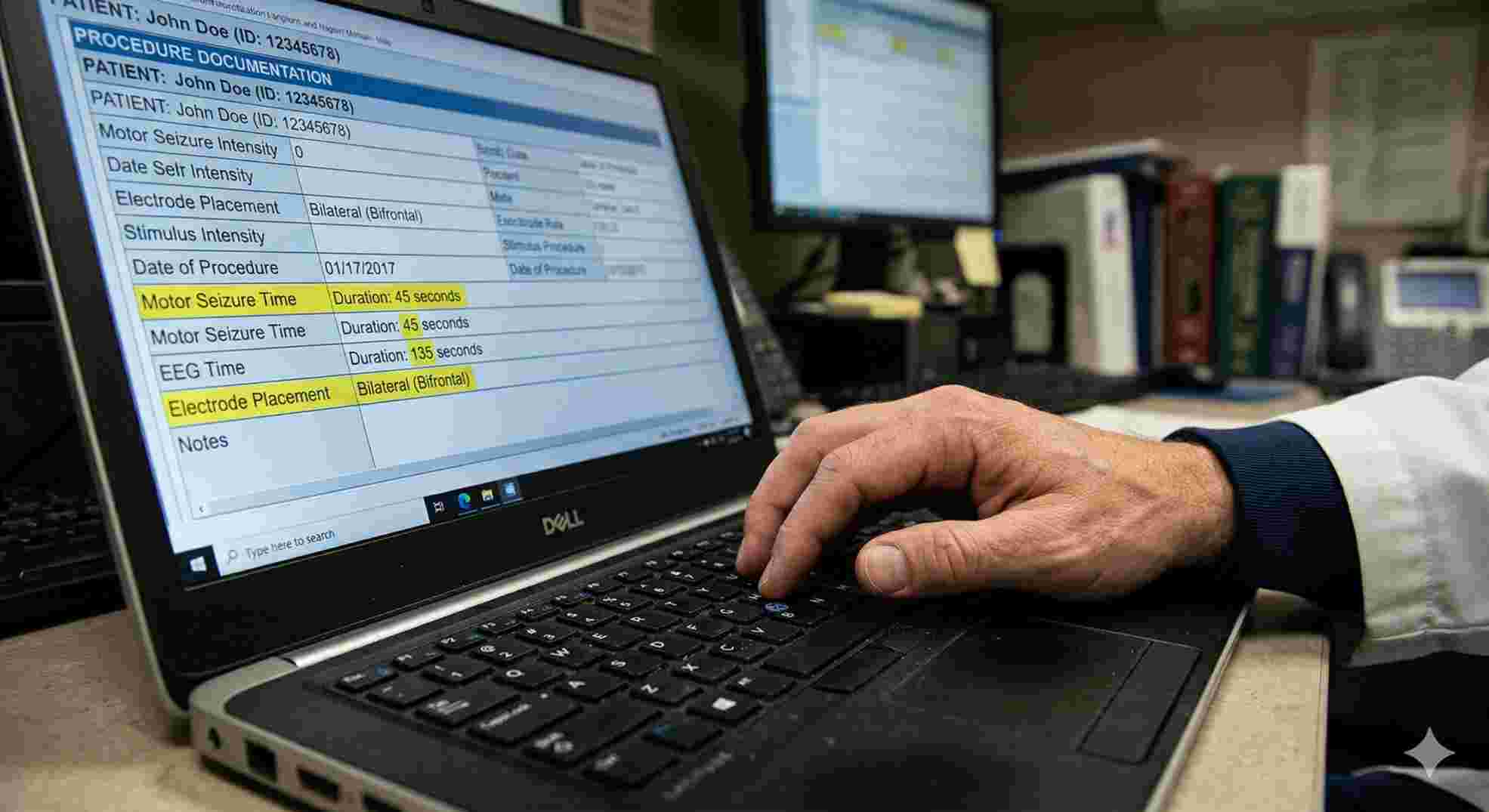
Generic operational notes frequently fail Medicare audits. Charting must be rigorous, numeric, and highly specific to validate the claim.
4. Establishing Medical Necessity in Behavioral Health Billing
Because electroconvulsive therapy is a high-acuity intervention, payers require robust medical necessity documentation. The ICD-10 diagnosis code must clinically justify the procedure.
| ICD-10 Code Group | Clinical Condition | Payer Audit Risk | Documentation Required for Approval |
|---|---|---|---|
| F32.x | Major Depressive Disorder (Single Episode) | High | Explicit documentation showing the failure of multiple psychopharmacology trials. |
| F33.x | Major Depressive Disorder (Recurrent) | Low | Accepted when severe or psychotic features are present in the clinical chart. |
| F31.x | Bipolar Disorder | Medium | Supported by the presence of severe, unmanageable manic or depressed phases. |
| F20.x | Schizophrenia | Medium | Well-supported when the patient exhibits acute catatonia. |
Intake histories must clearly outline treatment resistance, detailing specific medication trials, dosages, and the reasons for failure. Claims adjusters review these narratives to ensure the intervention meets the payer’s specific threshold for care.
5. Prior Authorization and Frequency Guidelines
Commercial health plans and Medicare Advantage networks heavily regulate psychiatric interventions. Facilities must secure strict prior authorization before initiating treatment.
Authorization requests generally cover a specific block of sessions, typically 6 to 12 treatments for an acute phase. Additionally, billing software must monitor frequency limitations. The standard industry guideline is three sessions per week. Variations from this schedule, such as step-down maintenance therapy, must be accompanied by detailed clinical reasoning.
6. Appropriate Place of Service (POS) Codes
Due to the necessity of general anesthesia, this procedure requires specialized facility infrastructure. Billing these services in a standard outpatient therapy office (POS 11) is non-compliant and routinely triggers payer investigations.
| Location / Provider Entity | Specific Service Billed | Billing Form Required |
|---|---|---|
| Attending Psychiatrist | CPT 90870 | CMS-1500 |
| Anesthesiologist | CPT 00104 | CMS-1500 |
| Hospital / Outpatient Facility | Revenue Code 0901 | UB-04 |
Compliant billing typically requires POS 21 (Inpatient Hospital) or POS 22 (On-Campus Outpatient Hospital). Facilities must coordinate internal billing departments to ensure that both the professional CMS-1500 claims and the facility UB-04 claims are submitted simultaneously.
7. Navigating Payer Audits and Claim Denials
Even with rigorous preparation, rejections occur. Developing an operational defense against standard denial codes is essential for maintaining cash flow.
Addressing Missing Modifier Denials
When a psychiatrist performs a standard Evaluation and Management (E/M) service and the psychiatric procedure on the same day, payers will bundle the claim unless correctly modified. Appending Modifier 25 to the E/M code (e.g., 99222) indicates that the evaluation was a significant, separately identifiable service. Providers must maintain two distinct clinical notes to support the use of Modifier 25.
Overcoming Medical Necessity Rejections
If a payer algorithm rejects a claim based on medical necessity, facilities must initiate a formal appeal. This process involves submitting the patient’s comprehensive medication history, highlighting failed pharmacological trials, and referencing the payer’s published medical policies.
Resolving Date Mismatch Errors
Date discrepancies between the psychiatric claim and the anesthesia claim result in automatic denials. Implementing internal hard stops—requiring manual verification of dates of service, patient demographics, and diagnosis codes before batch submission—eliminates this administrative error.
Official Industry References
- Centers for Medicare & Medicaid Services (CMS): Official Medicare Coding & Billing Guidelines
- American Medical Association (AMA): CPT® Procedure Code Resources
- American Psychiatric Association (APA): Clinical Parameters for Electroconvulsive Therapy
Running a behavioral health facility is exhausting enough without fighting insurance companies for the money you already earned. Every denied claim, coding error, or delayed prior authorization directly drains your cash flow and pulls your focus away from patient care. You need a dedicated financial team that actually understands the strict, highly audited clinical requirements of psychiatric billing. Stop leaving your revenue to chance. Partner with specialized experts who know how to protect your bottom line and get your complex claims paid on the very first submission.
