
You just pulled this week’s denial report. Another batch of rejected claims for a cpt code physical exam. It hurts to look at. You did the work, the patient got the care, but the insurance company refuses to cut the check.
Billing for preventative visits should be easy revenue. Instead, it turns into a massive headache of audits and patient complaints. You cannot afford to guess here. You need strict rules. This guide strips away the confusion and shows you exactly how to code these encounters so you actually get paid.
The Core Difference: Preventative vs. Problem-Oriented Visits
I stepped into a primary care clinic a few years back to help fix a cash flow crisis. The doctors were furious. They had billed hundreds of standard physicals to Medicare, and almost every single one bounced. Worse, their elderly patients suddenly started getting $200 bills in the mail. The clinic’s Google reviews tanked in a matter of weeks.
We dug into the charts. The problem hit me instantly. Patients were calling and asking for an “annual physical.” The front desk booked exactly that. The doctors did a head-to-toe exam and dropped a 99397.
But Medicare does not pay for routine physicals. They pay for the Annual Wellness Visit (AWV).
The clinic was treating a Medicare patient like a commercial patient. Once we fixed that single blind spot—and trained the front desk to screen those calls—the denials stopped entirely. You must know the cpt coding meaning for each visit type. A sick visit treats a specific problem. A preventative visit focuses on screening. Mix them up, and you lose money. For more context, you can review the official CMS guidelines on Medicare Annual Wellness Visits.
Complete List of Preventative Medicine CPT Codes
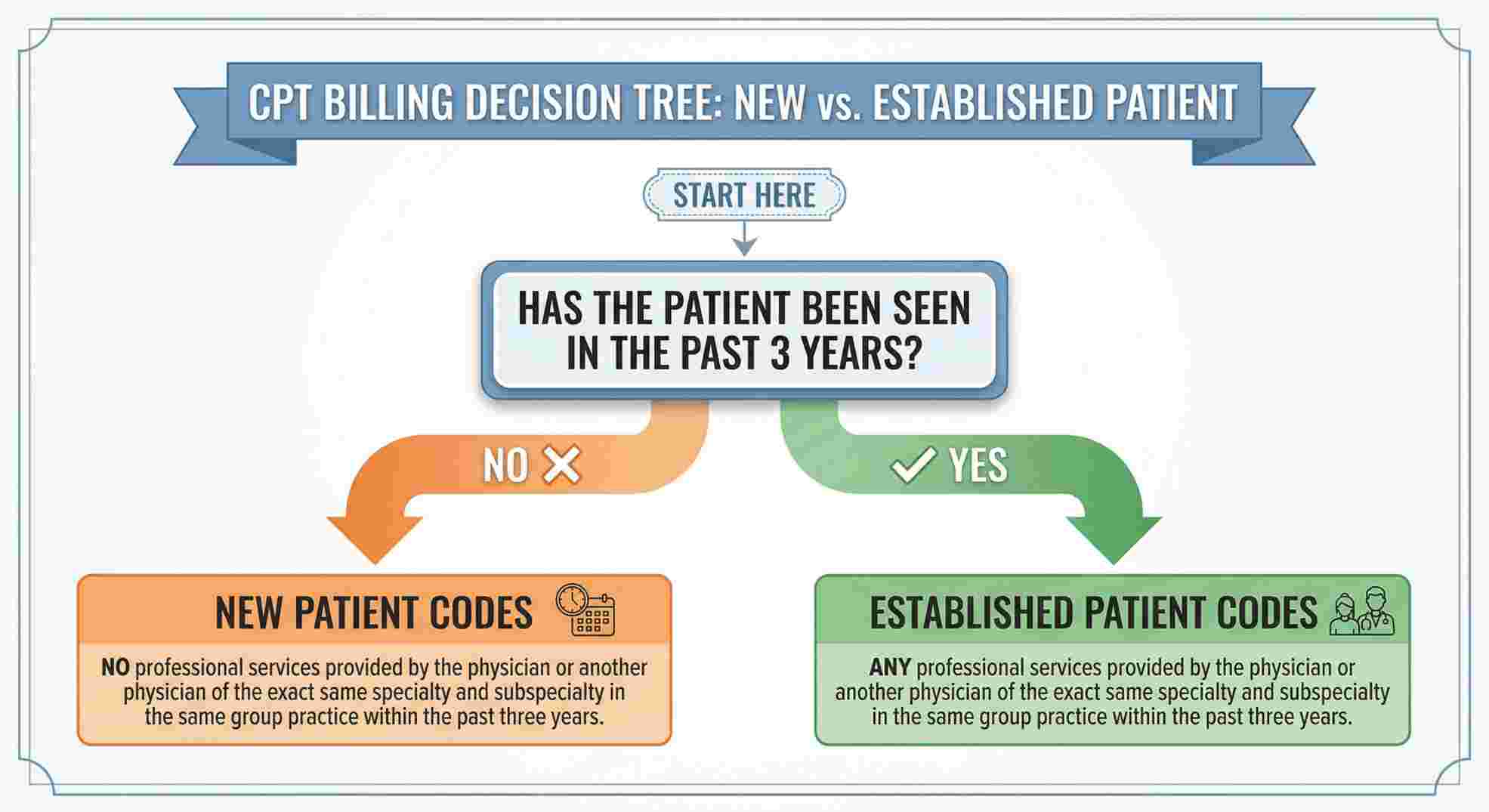
For your non-Medicare patients coming in for a check-up, you use the standard preventative medicine codes. You pick the code based on two things: how old the patient is, and whether they are a new or established patient.
Your billing team needs this list of cpt codes memorized.
| Patient Age | New Patient Code | Established Patient Code |
|---|---|---|
| Under 1 year | 99381 | 99391 |
| 1 to 4 years | 99382 | 99392 |
| 5 to 11 years | 99383 | 99393 |
| 12 to 17 years | 99384 | 99394 |
| 18 to 39 years | 99385 | 99395 |
| 40 to 64 years | 99386 | 99396 |
| 65 years and older | 99387 | 99397 |
A new patient is someone you have not seen for professional services in the past three years. If they came in two years ago, they are established. Get this wrong, and the claim dies.
Finding the Exact cpt code physical Exams Require
A cpt code definition is simply your way of talking to the payer.
When you submit codes 99381 through 99397, you are making a promise. You are promising that the doctor did a comprehensive history, a full exam, and provided counseling. If the chart notes just say “Listened to heart, patient feels fine,” you cannot bill these codes. An auditor will take that money right back. Proper documentation always aligns with the AMA guidelines on Preventative Medicine Services.
Medicare Annual Wellness Visits (AWV) vs. Routine Physicals
Medicare plays by a completely different rulebook.
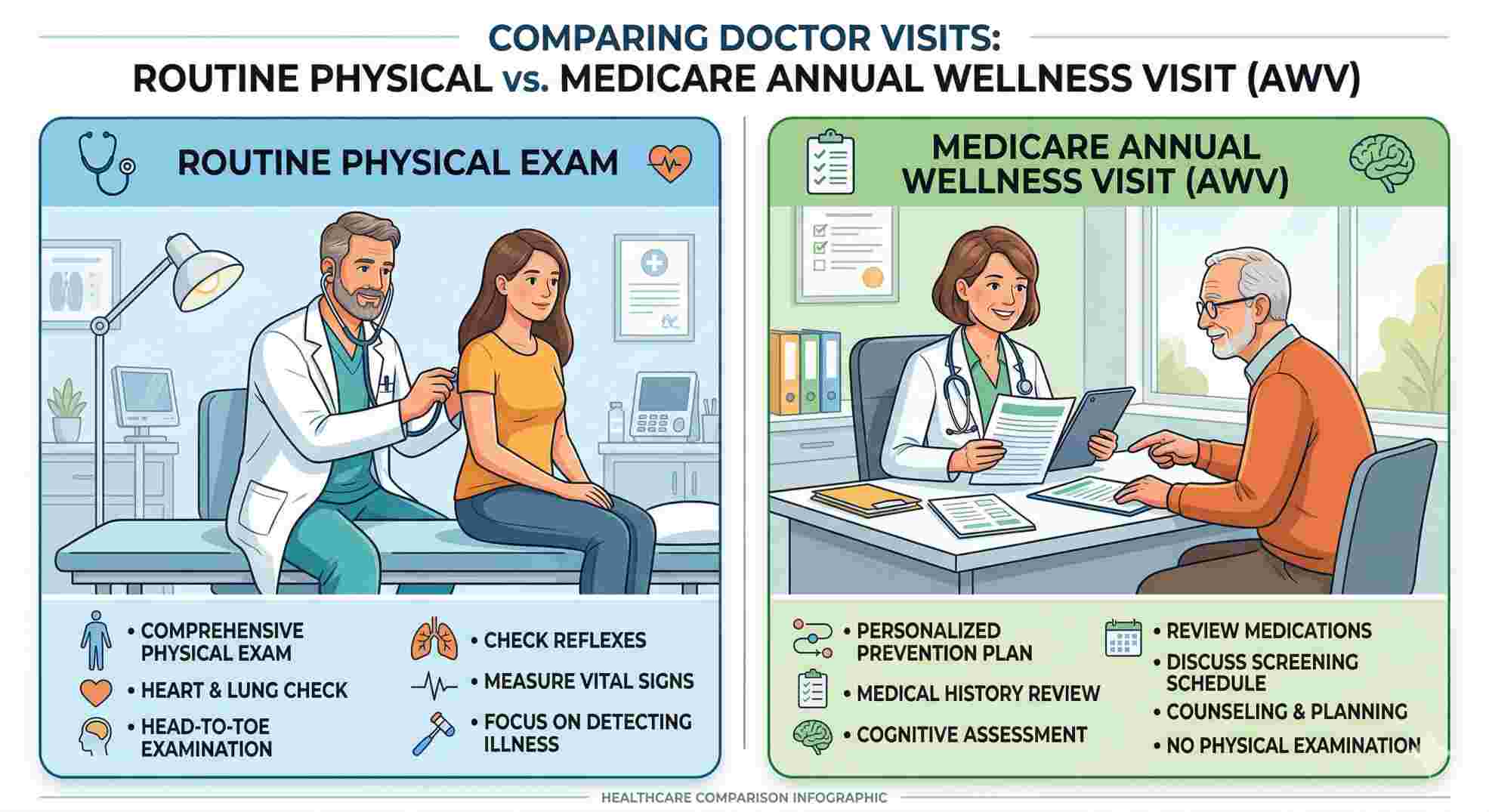
They do not want a physical exam. They want a cognitive exam. The AWV is about sitting down with the patient, reviewing their medical history, checking for fall risks, and creating a preventative plan. You must train your providers to stop doing hands-on physicals when billing an AWV.
| Feature | Routine Physical (Commercial) | Medicare AWV (Medicare) |
|---|---|---|
| Primary Codes | 99381 – 99397 | G0438, G0439 |
| Main Focus | Hands-on physical exam | Health risk assessment & planning |
| Patient Cost | Usually $0 (under ACA) | $0 copay |
| Vitals Required | Yes | Yes (Height, weight, BP, BMI) |
| Cognitive Focus | Low to Moderate | High (Screening for depression, falls) |
Submit a 99397 to Medicare, and it will fail. Use G0438 for the patient’s very first AWV. Use G0439 for every year after that.
Using Modifier 25 During a Routine Physical
Patients always bring up new problems during a physical. They come in for a check-up, but then ask the doctor to look at a painful knee, or they break down and discuss severe anxiety and depression.
You can bill for both the physical and the sick visit. But you have to use Modifier 25.
Modifier 25 tells the payer that the doctor did extra, significant work on top of the preventative visit. You attach this modifier to the sick visit code (like a 99213).
| Factor | Description | Impact on Practice |
|---|---|---|
| Pro | Increased Revenue | You get paid for all the work you actually did. |
| Pro | Patient Convenience | The patient avoids coming back for a second visit. |
| Con | Audit Target | Insurance payers heavily audit this modifier. |
| Con | Strict Documentation | Providers must write two separate notes to prove the extra work. |
Do not fake this. If the doctor just writes a quick refill prescription, that is not enough to bill a separate visit. Furthermore, if your primary care practice is starting to integrate more behavioral health screenings, the coding rules change completely. You cannot treat psychiatric CPT codes like standard E/M codes. For a closer look at those specific compliance traps, you need to understand The Real Truth About Coding and Billing for Mental Health Services.
It is highly recommended to study the OIG compliance guidelines for Modifier 25 to avoid aggressive audits across all these visit types.
Common CPT Codes for Physical Therapy Evaluations
Physical therapy clinics follow a different set of rules. If someone asks about common cpt codes for physical therapy, they mean evaluations, not preventative physicals.
A PT evaluation depends entirely on the complexity of the patient’s condition.
- 97161: Low complexity PT evaluation.
- 97162: Moderate complexity PT evaluation.
- 97163: High complexity PT evaluation.
You have to get the diagnosis vs procedure code match right. The diagnosis code shows why the patient is there. The procedure code shows what you did. If those two do not make sense together, your claim goes in the trash. Always consult the latest APTA guidelines on physical therapy evaluation codes when building your clinical notes.

5 Proven RCM Strategies to Prevent Physical Exam Denials
Knowing the billable cpt codes is just step one. Your front office workflow decides if you actually see the money. Run these five plays.
Strategy 1 & 2: Front Desk Operations
1. Script the Front Desk
Your front desk must clarify what the patient wants. If an older patient says “physical,” staff must explain the Medicare AWV immediately before booking.
2. Check Benefits Three Days Out
Never guess. Check eligibility 72 hours before the visit. Find out exactly which codes are covered and if the patient owes a copay.
Strategy 3: Technical Failsafes
3. Use EMR Hard-Stops
Build rules into your software. If a doctor tries to send a commercial code to Medicare, the system should freeze and demand a correction.
Strategy 4 & 5: Back-Office Communications
4. Lock Down Your Intake Emails
Bad communication causes billing errors. Tell your intake team to gather updates at hello@dmedevices.com. Keep everything in one place.
5. Clean Up Your Vendor Contacts
If you outsource billing, ensure they get denial alerts instantly. Update your internal routing email from primellc.digital@gmail.com. Missing a deadline because of an old email address is a rookie mistake.