

You have a patient in front of you who is clearly suffering, and finding the right adjustment disorder code dsm classification is likely the last thing on your mind—until you have to bill for it. They aren’t clinically depressed in the biological sense, and they don’t have a generalized anxiety disorder. But their life just fell apart—maybe a divorce, a layoff, or a medical scare—and they are struggling to cope. You know what it is. But when you go to billing, you freeze. Which code actually gets paid?
It’s a headache. You’re staring at the screen, toggling between F43.21 and F43.20, wondering if you’re about to trigger an audit. The shift from the old manuals to the current system didn’t make this easier; it just added more layers of red tape.
We are going to fix that. Right now. No fluff, no academic lectures. Just the exact logic you need to pick the right code, get your claim approved, and get back to seeing patients.
The “Lightbulb” Moment: You Don’t Bill the Book
Here is the thing that trips up almost every new therapist I supervise. You are looking for an adjustment disorder code dsm in the manual, but the DSM doesn’t technically have billing codes.
The DSM-5 gives you the criteria (the symptoms).
The ICD-10 gives you the code (the money).
The DSM-5 is just a bridge. It describes a condition and then points you to an ICD code (like F43.21). Why does this matter? Because insurance companies don’t care about your clinical nuance; they care about the alphanumeric string on Box 21 of the claim form. If you diagnose based on the DSM but use a “rule-out” or vague code that doesn’t match the ICD-10 specifics required by CMS, you are essentially working for free.
The Primary Categories (And How to Pick One)
Adjustment disorders used to be the “wastebasket” diagnosis. Not anymore. Now, classified under Trauma- and Stressor-Related Disorders, they have teeth.
To find the right adjustment disorder code dsm, you have to look at the dominant symptom. What is the loudest emotion in the room?
The Rules of the Road
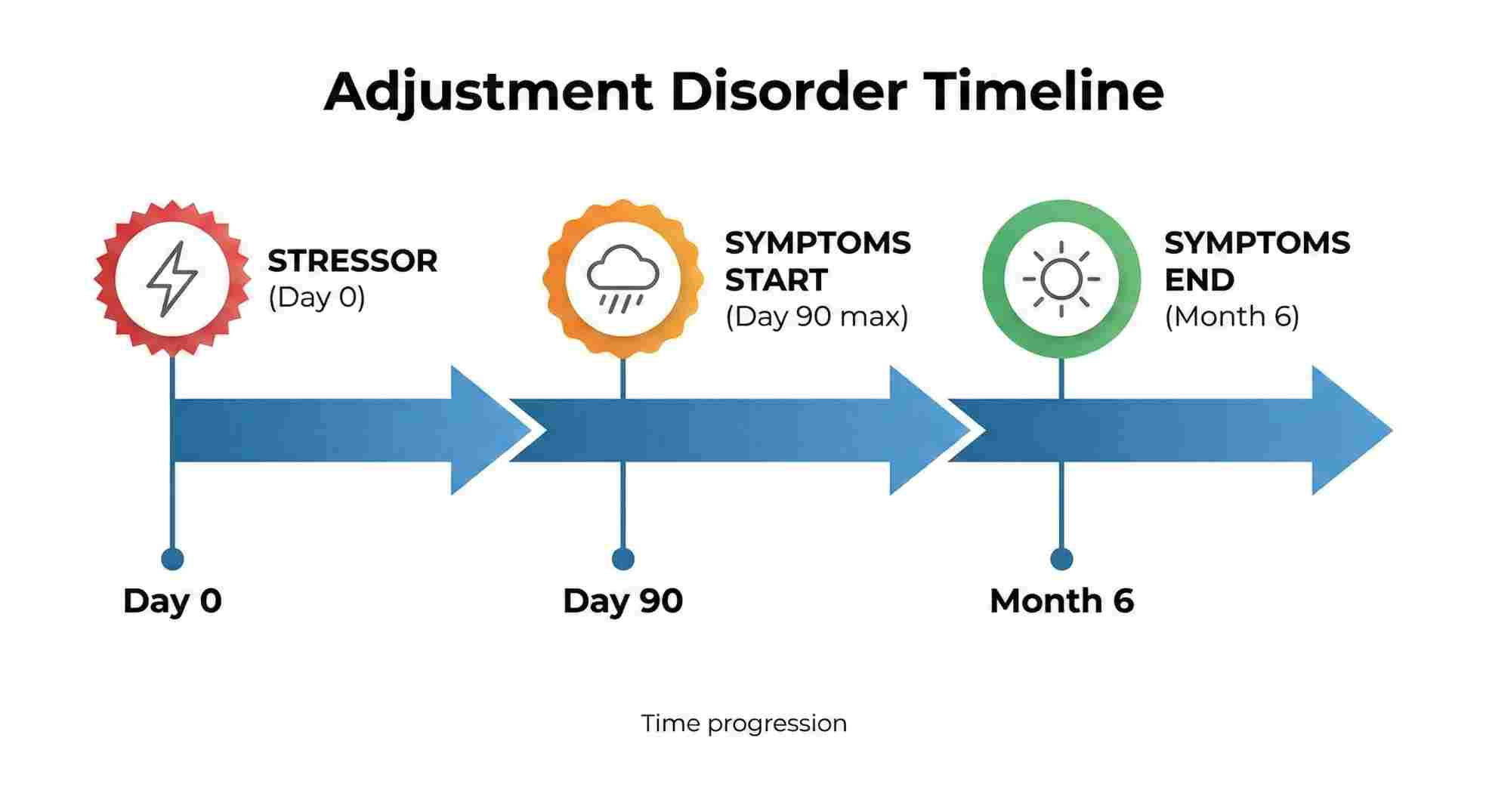
Before you even touch a code, check these three boxes:
- The Clock: Symptoms started within 3 months of the stressor.
- The Impact: The distress is bigger than what you’d normally expect, OR it’s messing up their job/relationships.
- The Limit: Once the stressor stops, the symptoms can’t last more than 6 months.
The Codes You Will Use Daily
You don’t need to memorize the whole book. You need these five.
F43.21: The “Sad” One
If your client is crying, feels hopeless, or just can’t get off the couch after a breakup, this is it. The adjustment disorder with depressed mood f code is F43.21.
Real talk: Don’t use this if they meet the full criteria for Major Depression. This is for situational sadness.
F43.22: The “Nervous” One
- Code: F43.22 (With Anxiety)
- Signs: They are jittery, worried, or stressed out about the event.
- Example: A guy who got fired and now has panic attacks whenever he opens LinkedIn, but was fine before the firing.
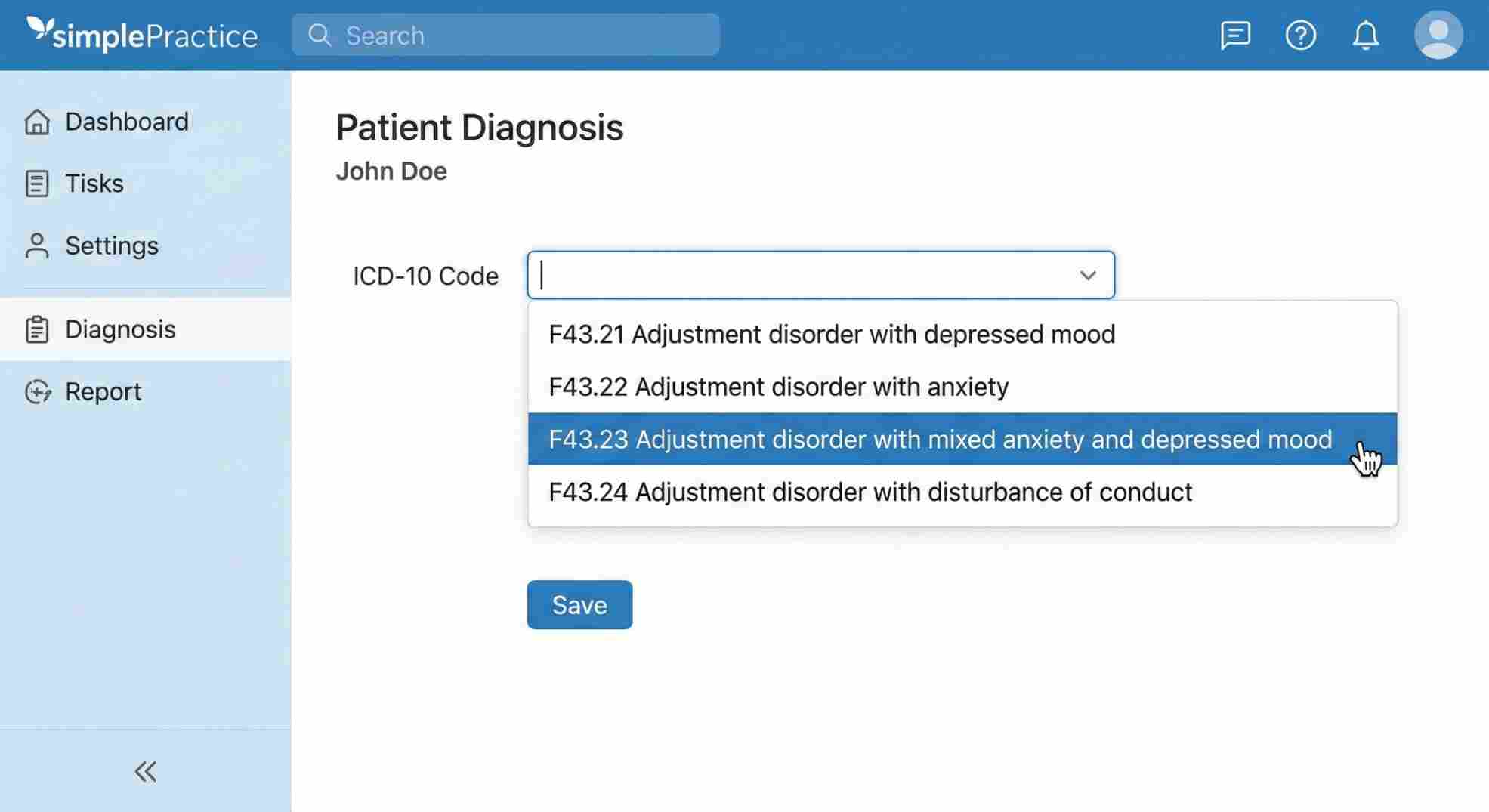
F43.23: The Combo Platter
- Code: F43.23 (Mixed Anxiety and Depressed Mood)
- Why use it: Honestly? This is the most accurate code for 80% of humans. Most people aren’t just “sad” or just “anxious”—they are a messy mix of both.
F43.24: The “Acting Out” One
- Code: F43.24 (With Disturbance of Conduct)
- Signs: This is usually for teens. Skipping school, vandalism, reckless driving. The emotional pain is coming out as bad behavior.
F43.20: The Vague One (Avoid This)
The adjustment disorder nos code is F43.20.
My advice: Don’t use it unless you have a gun to your head. Insurance payers hate “unspecified” codes. It looks like you didn’t do a thorough assessment. Only use this if the symptoms are weird and don’t fit the other boxes.
Cheat Sheet: Criteria to Code
I keep a version of this taped to my desk. It saves me five minutes of Googling every day.
Table 1: Clinical Symptom Map
| DSM-5 Specifier | What You See in the Room | ICD-10 Code |
|---|---|---|
| With Depressed Mood | Tears, hopelessness, low energy. | F43.21 |
| With Anxiety | Jitters, worry, heart racing. | F43.22 |
| Mixed Anxiety & Depression | A little bit of both. | F43.23 |
| With Conduct Issues | Breaking rules, fighting, truancy. | F43.24 |
| Mixed Emotion & Conduct | Sad/anxious AND acting out. | F43.25 |
| Unspecified | Doesn’t fit the above. | F43.20 |
Old School vs. New School (DSM-IV vs. ICD-10)
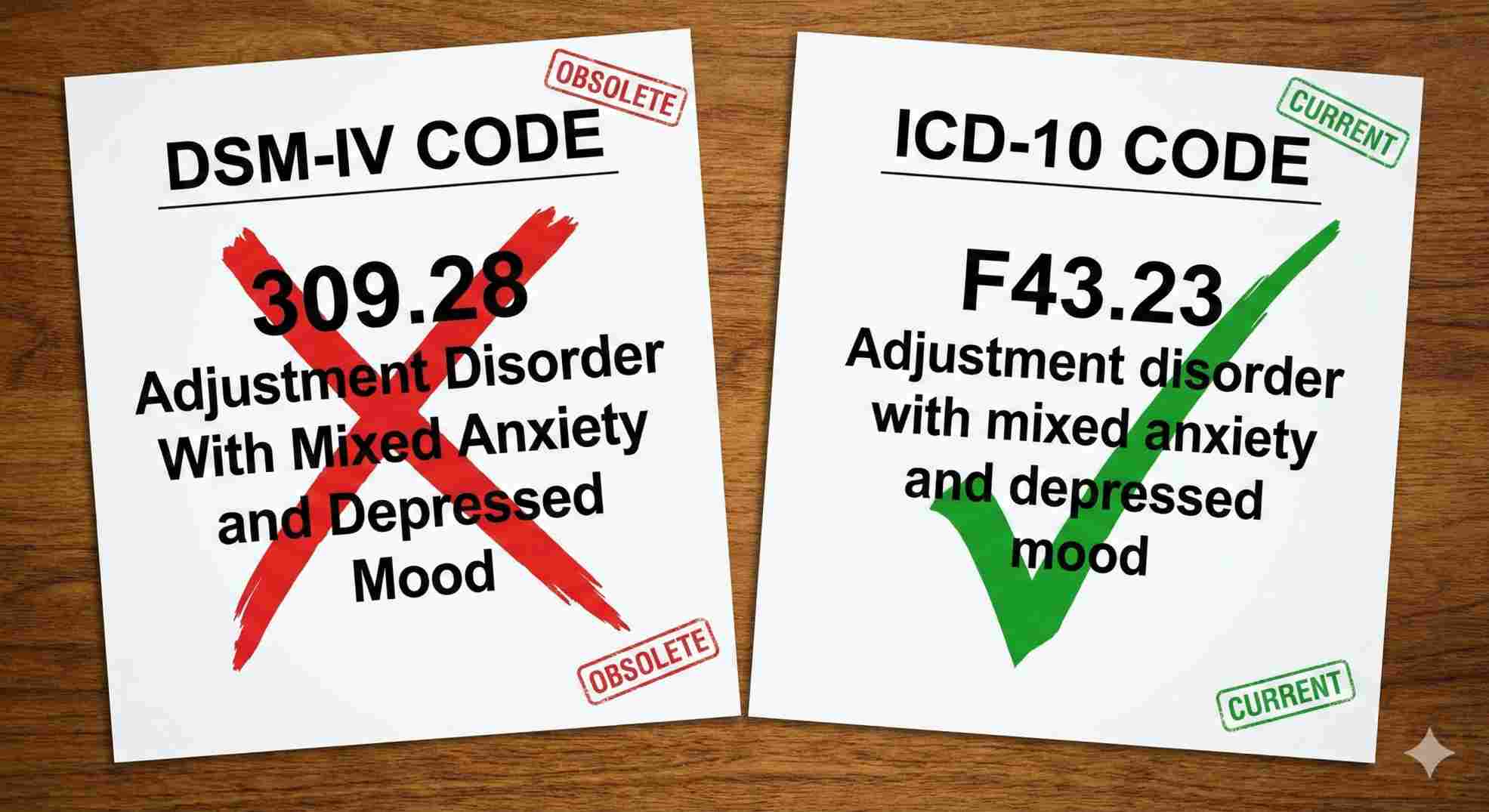
If you have been in the game a long time, you might remember the “309” codes. You need to forget them. The adjustment disorder dsm iv code set is dead.
If you submit a claim with “309.0” today, the computer system at Blue Cross will reject it in milliseconds. We live in the “F-code” era now.
Table 2: The Translation Guide
| If you used to write… | You MUST now write… |
|---|---|
| 309.0 (Depressed) | F43.21 |
| 309.24 (Anxious) | F43.22 |
| 309.28 (Mixed) | F43.23 |
| 309.3 (Conduct) | F43.24 |
| 309.9 (Unspecified) | F43.20 |
Why Claims Get Denied (And How to Fix It)
I’ve seen practices lose thousands of dollars because they got lazy with the adjustment disorder code dsm specifics. Here is where things go wrong.
1. The “Ghost” Stressor
You diagnosed an adjustment disorder, but your note doesn’t say what they are adjusting to.
- Fix: Your intake note must name the event. “Patient struggling with recent divorce finalization.” If there is no event, it’s not an adjustment disorder.
2. The “Forever” Patient
You have been billing F43.21 for two years.
- The Problem: Remember the 6-month rule? If the stressor is over, the diagnosis expires. If they are still depressed a year later, that is likely Major Depressive Disorder now. Update your treatment plan.
3. The Mismatch
You billed F43.24 (Conduct Disturbance) but your note only talks about crying.
- The Result: Audit failure. The story in your notes has to match the title of the chapter (the code).
Table 3: Denial Prevention
| The Error | Why It Fails | Quick Fix |
|---|---|---|
| Time Limit Exceeded | Code used >6 months past stressor. | Re-evaluate. Is it MDD or GAD now? |
| Vague Coding | Using F43.20 (Unspecified) too often. | Pick a specific symptom (Anxiety/Depression). |
| No “Index Event” | No stressor listed in notes. | Write down exactly what happened to the patient. |
Treatment: What This Code Tells the Payer
When you use an adjustment disorder diagnostic code, you are sending a signal to the insurance company. You are telling them: “This is situational. It will get better. We don’t need 5 years of analysis.”
This code usually justifies a short, sharp course of therapy—maybe 8 to 12 sessions of CBT or solution-focused work. If you try to request 50 sessions upfront with an F43 code, you’re going to get a phone call from a case manager asking what is going on.

Final Thoughts
Getting the adjustment disorder code dsm right isn’t just about satisfying the bureaucrats. It’s about clarity. It’s about looking at another provider’s notes and knowing exactly what that patient was going through at that moment in time.
Avoid the vague adjustment disorder nos code unless you have no choice. Be specific. identifying the stressor, checking the timeline, and matching the symptoms to the right F-code. It sounds boring, but accuracy here is what keeps your doors open and your practice safe. If you need a deeper dive on how this fits into your broader revenue cycle, check out our full guide on The Real Truth About Coding and Billing for Mental Health Services.
Now, go check your last few notes. Did you use the right code? If not, fix it now. Future you will appreciate it.