You are probably losing money on mental health screenings right now. I see it happen every single week. Medical clinics do the hard work of screening patients for mental health risks, only to get slapped with claim denials because their cpt 96127 documentation requirements are a complete mess. It is incredibly frustrating to provide good patient care and then watch the insurance company refuse to pay over a minor charting technicality.
Right now, the push for behavioral health integration in primary care is massive. You want to catch issues early. But payer scrutiny is tighter than ever. Insurance companies are no longer just approving these claims automatically. They have aggressive audit programs specifically targeting brief behavioral assessments, and they are actively looking for reasons to claw back their money. In fact, if you want to survive these audits, mastering this single code is just step one in the much larger puzzle of coding and billing for mental health services.
We have to fix this broken system in your practice. By tightening up exactly how your clinical team writes these specific chart notes, you can bulletproof your revenue. Let’s break down the exact rules, the payer expectations, and the daily charting habits you need to get these claims paid the first time, every time.
The “Four-Point” Defense Strategy for Audits
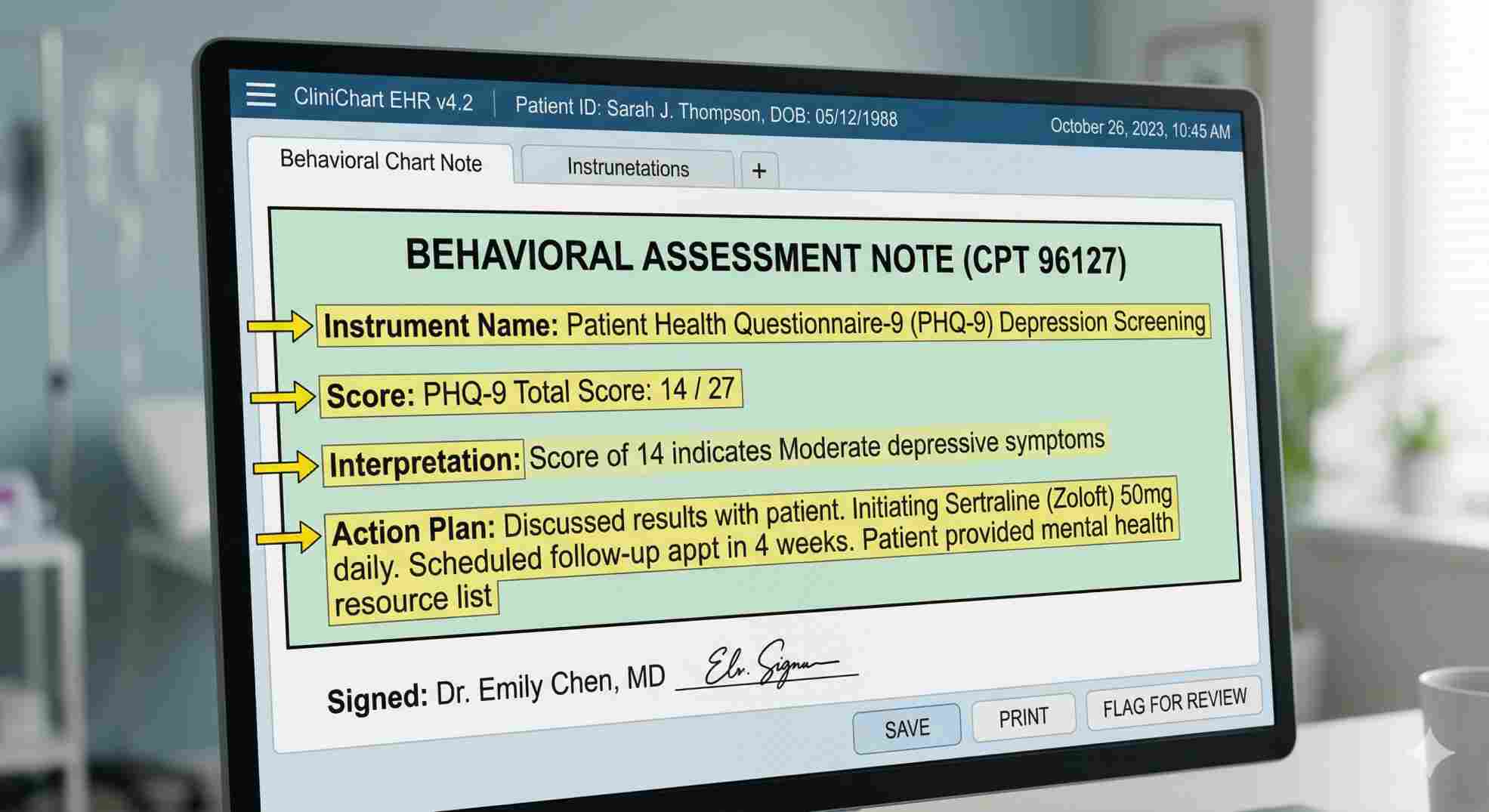
Here is the harsh reality that most billers miss. An auditor does not care how long you talked to the patient about their feelings. To pass an audit and keep your money, every single note for this code needs exactly four things: the name of the test, the numerical score, a quick interpretation, and your clinical plan. That is it. If your current EHR setup does not force your doctors to type those four specific things, you are highly vulnerable. Mastering cpt 96127 documentation requirements means refusing to close a chart until those four data points are clearly visible.
Breaking Down the 96127 CPT Code Description
To bill this correctly, you need to understand the exact coding rules. According to the American Academy of Professional Coders (AAPC), the official 96127 cpt code description calls for a “brief emotional/behavioral assessment… with scoring and documentation, per standardized instrument.”
Look closely at those words. “Brief” means this is a quick screen, not a full psychiatric workup. “Standardized instrument” is the trap most doctors fall into. You cannot just ask a teenager how school is going, write down “patient seems anxious,” and bill the code. You have to use a recognized, validated questionnaire that gives you a hard number at the end.
You are getting paid for the administration of the test, scoring the math, and taking the time to write down what those numbers mean for the patient’s health.
Non-Negotiable CPT 96127 Documentation Requirements
Guessing what an insurance adjuster wants to see is a bad business model. You need strict, unbreakable templates.
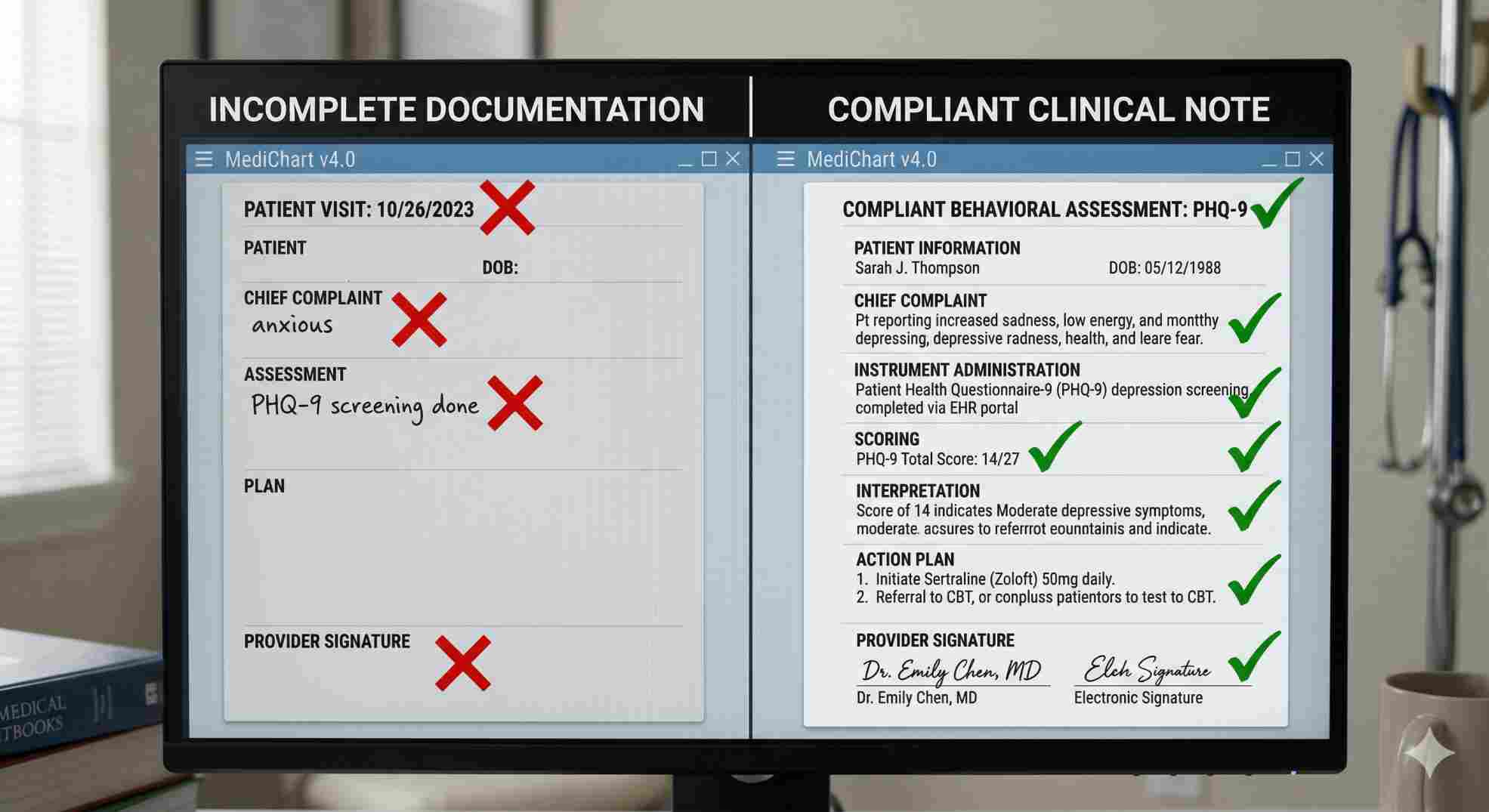
When an auditor pulls your files, they want a clear story. They want proof that the test was necessary, that a real tool was used, and that the doctor actually looked at the results to make a medical decision. If your medical assistant hands the patient an iPad in the waiting room, and those results just quietly sit in the chart without the doctor ever bringing them up, you fail the audit.
Your notes must prove the provider was involved. Let’s look at exactly what fails and what passes when it comes to cpt 96127 documentation requirements.
Audit Defense Comparison
Table 1: Charting Examples
| Charting Element | What Gets Denied | What Gets Paid |
|---|---|---|
| Instrument Name | “Patient screened for depression.” | “Patient completed the PHQ-9 depression screening.” |
| Scoring | “Test was positive.” | “PHQ-9 score: 14/27.” |
| Interpretation | (Left blank) | “Score of 14 indicates moderate depressive symptoms.” |
| Action Plan | “Follow up in 3 months.” | “Initiating Zoloft 50mg. Referral sent for CBT. Follow up 4 weeks.” |
If you force your staff to use the paid examples above, your cpt 96127 documentation requirements are handled. You take the guesswork away from the auditor.
The Search for a CPT Code for Anxiety and CPT Code ADHD
Coders and doctors argue about this all the time. People constantly search manuals looking for a highly specific cpt code for anxiety or a dedicated cpt code adhd.
They don’t exist as separate codes for basic screening. The code is always 96127. The AMA uses this single code as a catch-all bucket for any brief, standardized mental health assessment.
For anxiety, clinics mostly use the GAD-7 tool. When the patient takes the GAD-7, you bill 96127. For ADHD, pediatricians lean on the Vanderbilt scales. When a teacher fills out that Vanderbilt form, you bill 96127.
Approved Standardized Instruments
Table 2: Codes by Condition
| Condition You Are Testing | The Paperwork You Use | The Code You Bill |
|---|---|---|
| Anxiety | GAD-7, SCARED | 96127 |
| ADHD | Vanderbilt, Conners, BASC-3 | 96127 |
| Depression (Commercial) | PHQ-9, BDI | 96127 |
| Substance Abuse | DAST-10, AUDIT | 96127 |
This makes billing easy, but it makes charting harder. Because one code covers so many different diseases, your cpt 96127 documentation requirements have to clearly state exactly which test you gave them.
Strict CPT 96127 Billing Guidelines
Writing a good note does not guarantee payment. You have to understand the math and the modifiers behind 96127 billing guidelines.
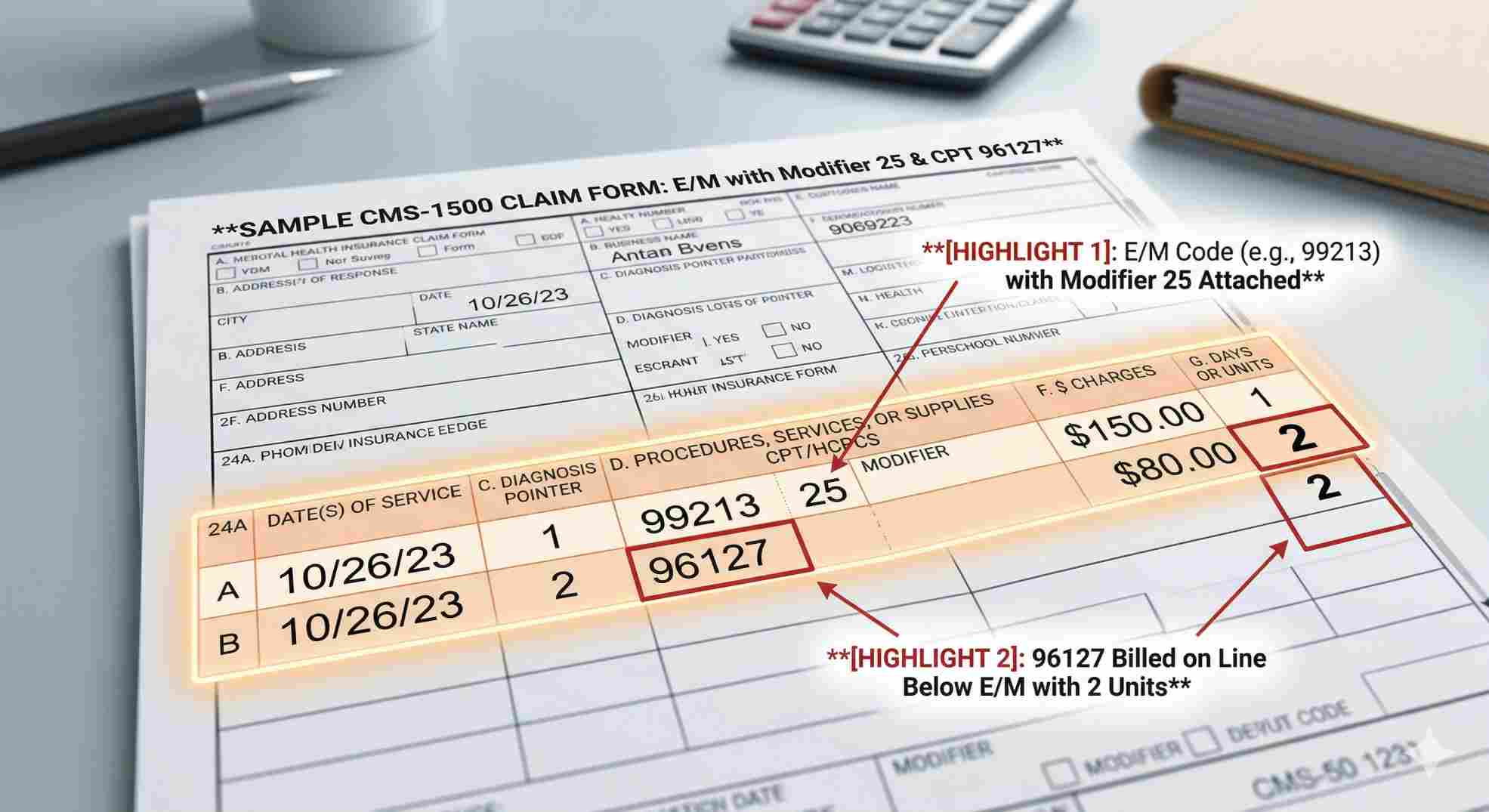
First, let’s talk about limits. You can bill this code multiple times per visit if you use different tests. If a patient takes a depression test and an anxiety test, you bill two units of 96127. But be smart. If you try to bill five units on one Tuesday afternoon, the insurance company will flag your account for an audit. Keep it reasonable. Most commercial plans cap you at three units per day.
Next is the modifier rule. You are almost always doing this screening during a normal doctor visit (like a 99213). To get paid for both, you must attach Modifier 25 to your main visit code. This proves to the payer that the mental health test was extra work, not just a normal part of a physical exam. Ignoring this rule is the fastest way to get denied. To satisfy 96127 billing guidelines, that modifier is your best friend.
The Trap of CPT 96127 Medicare Guidelines
Do not treat Medicare like a normal insurance company. If you do, you will lose money.
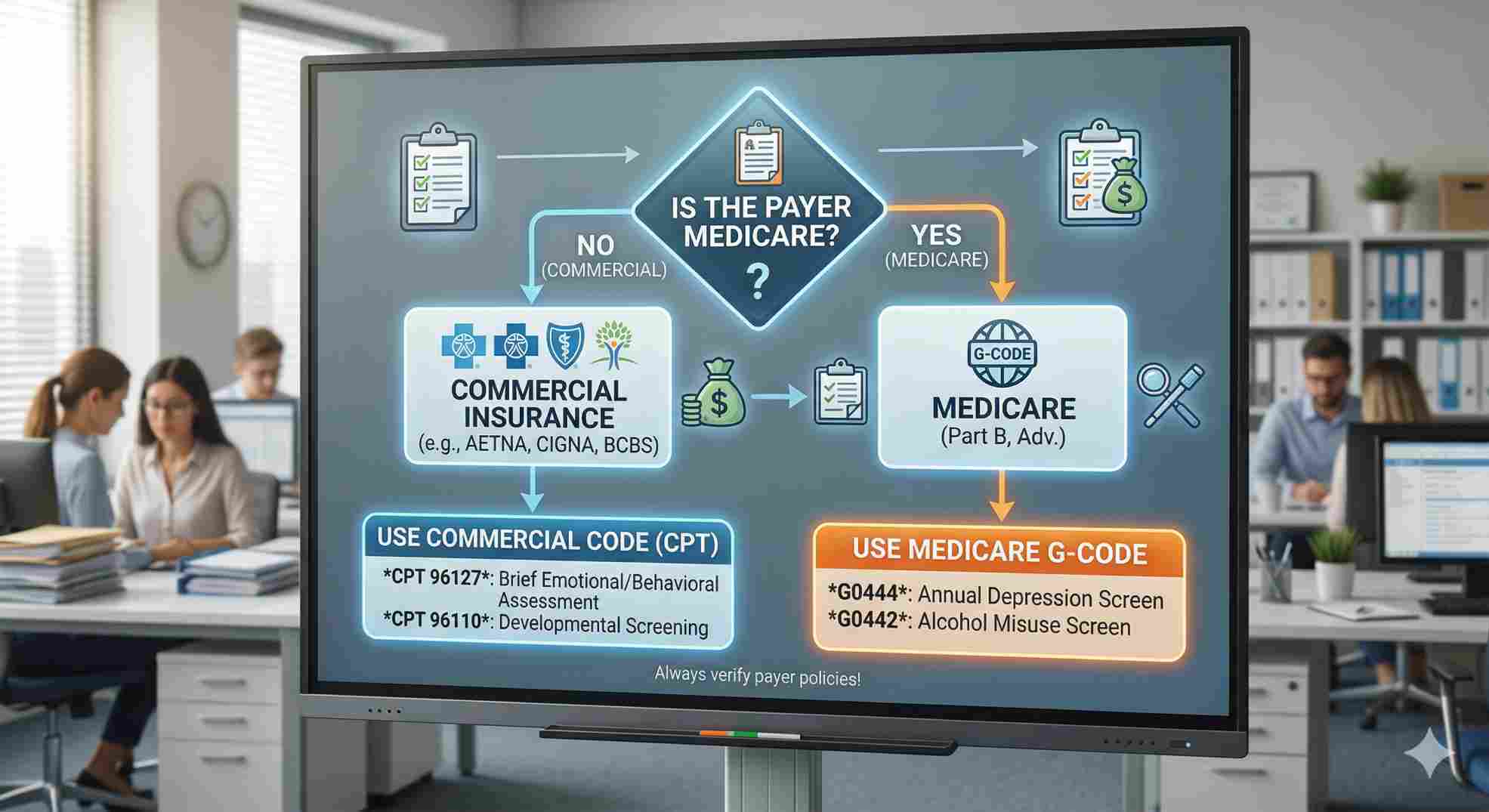
If you check the CMS Medicare Coverage Database, you will see the cpt 96127 medicare guidelines are totally different from commercial rules. Medicare likes to use their own specific “G-codes” for annual checkups. If you are doing a routine yearly depression screening on a 70-year-old patient, Medicare wants you to use G0444. If you use 96127 for that routine annual test, Medicare will deny it instantly.
Medicare usually only accepts 96127 if you are tracking a known problem, not just doing a broad annual screen.
Payer Rule Variations
Table 3: Commercial vs. Medicare
| Patient Scenario | Blue Cross / Aetna Rule | Medicare Rule |
|---|---|---|
| Annual Depression Screen | Bill 96127 | Bill G0444 |
| Tracking known Anxiety | Bill 96127 | Bill 96127 (if justified) |
| Units allowed | Usually up to 3 or 4 | Strictly watched, usually 1 or 2 |
Fixing Your Daily Clinical Workflow
You cannot expect busy doctors to remember all these rules while they have a waiting room full of sick people. You have to build cpt 96127 documentation requirements into your computers so they happen automatically.
Set up a shortcut in your medical software. When a doctor types a shortcut phrase like “.screen”, a blank box should pop up. It should have empty spots for the test name, the score, what the score means, and the medication or therapy plan.
If the doctor tries to close the chart without filling in those blanks, the system should stop them. When you take away the chance to make a mistake, your compliance goes to 100 percent. Your audits come back clean, and your bank account stays full.
Fighting Back Against Unfair Denials
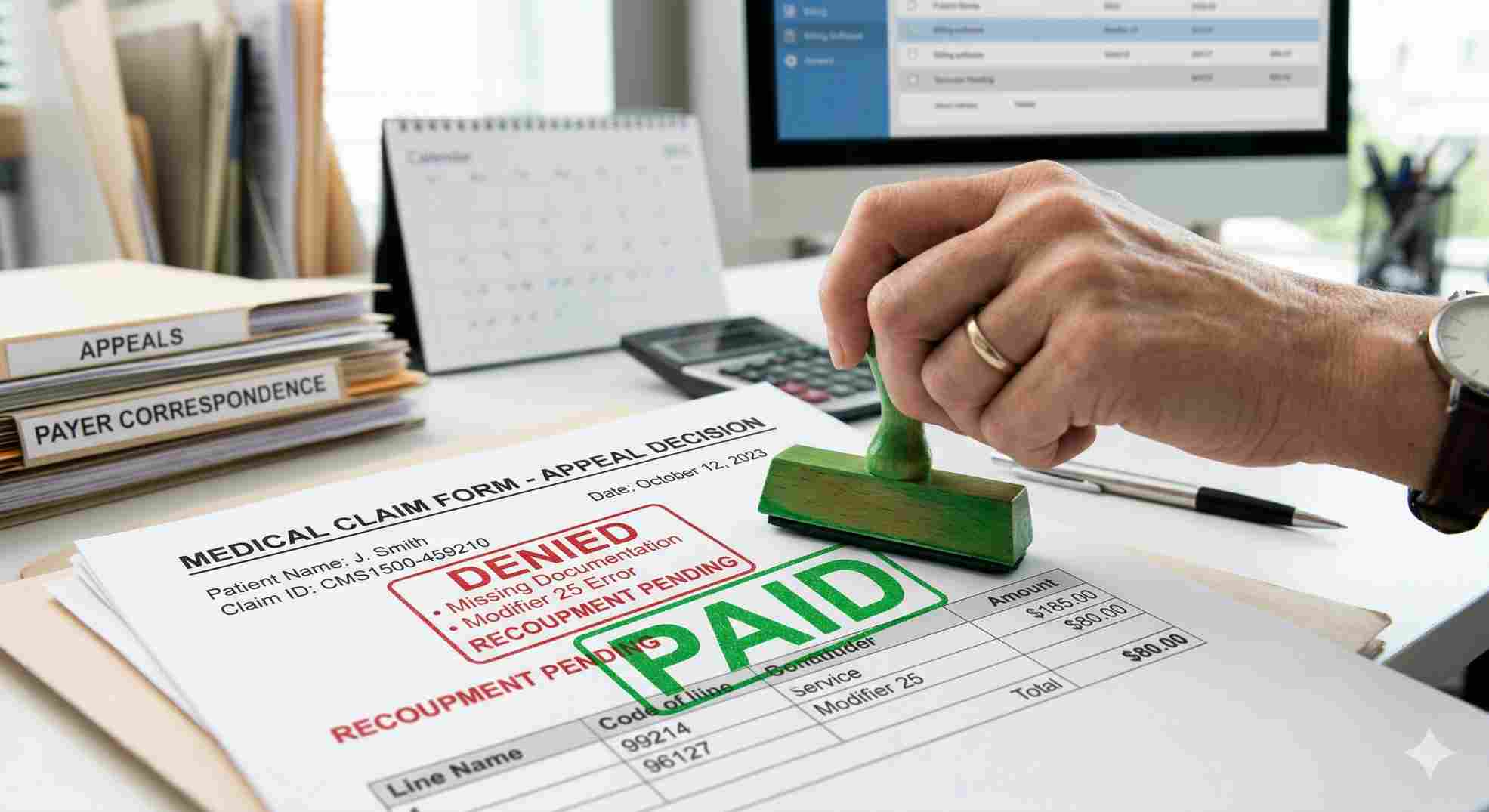
Even if your notes are perfect, insurance companies use automated software that will sometimes deny your claim anyway. They often use code CO-97, claiming the screening was just part of the normal visit.
Do not accept this. Fight back.
Print out your perfect chart note. Highlight the exact sentence where you met the cpt 96127 documentation requirements. Write a short, firm appeal letter stating that you provided a separate, necessary service and attached the right modifier. Insurance companies track which clinics roll over and which ones fight for their money. Be the clinic that fights.
You do the hard work of caring for patients. You deserve to get paid for it. Stop letting insurance companies dictate your revenue through technicalities. Fix your charting templates today, train your staff on exactly what to write, and enforce strict cpt 96127 documentation requirements across your entire practice. When you control the documentation, you control your business.