
You just opened your latest batch of clearinghouse reports, and there it is again—another rejected claim for the cpt code for ect. It is incredibly frustrating to watch thousands of dollars get tied up in administrative red tape simply because a commercial payer’s algorithm decided your documentation missed a minor detail.
Behavioral health margins are already tight. If you know the real truth about coding and billing for mental health services, you know that standard claims are hard enough to get paid. When insurance companies delay your electroconvulsive therapy payments for weeks or months, it drains your cash flow and forces your billing staff into an endless, exhausting cycle of phone calls and appeals. Right now, Medicare and private insurers are scrutinizing high-cost mental health treatments harder than ever before.
We are going to stop that cycle today. I am going to show you exactly how to submit the cpt code for ect so it gets paid on the first try, how to structure your clinical notes to pass any audit, and how to completely bulletproof your revenue cycle.
The Quick Win: The Anesthesia Trap That Kills Claims
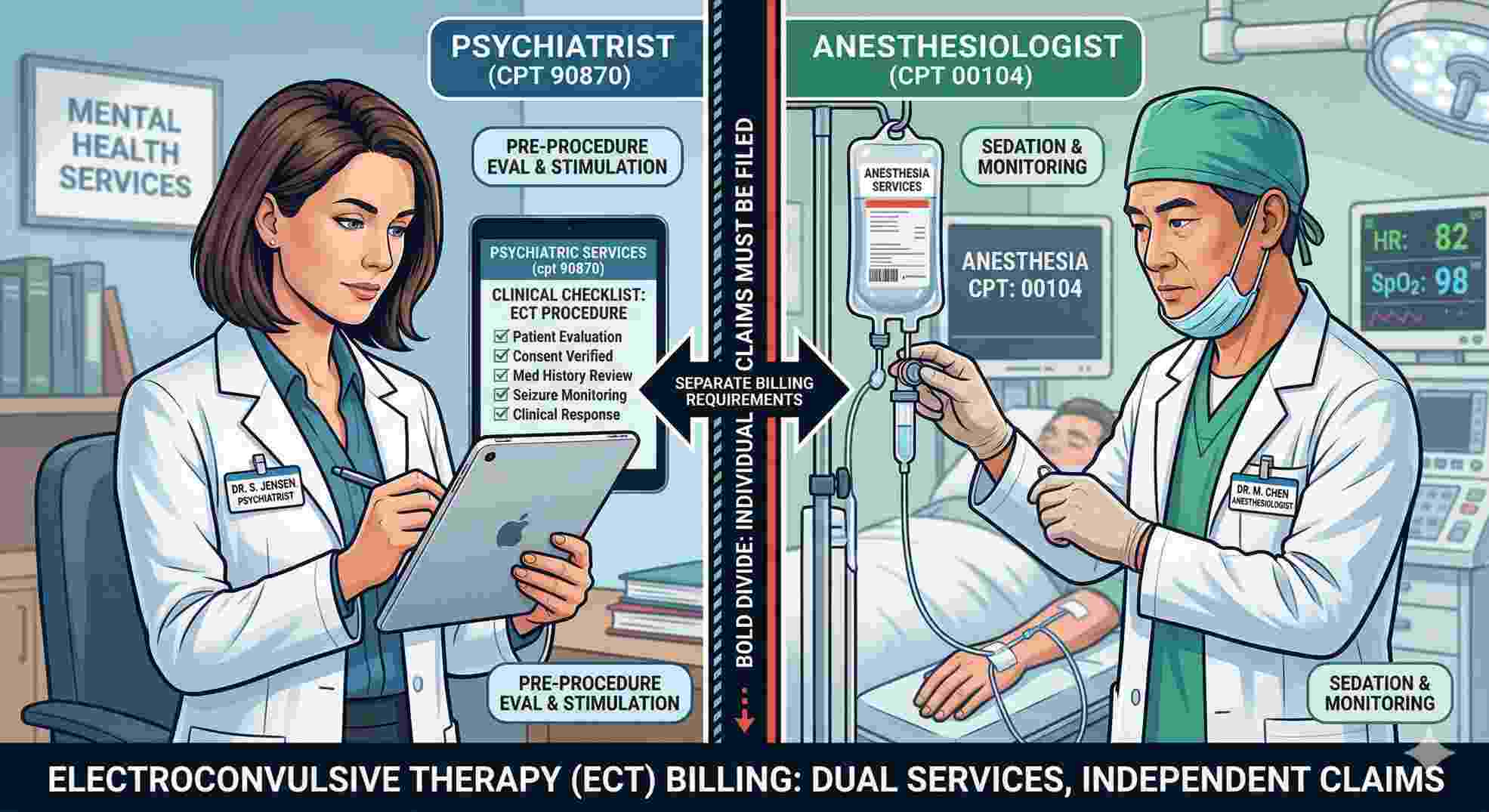
Let’s address the biggest leak in your billing process right away. The main reason practices fail when billing the cpt code for ect is a simple misunderstanding of what the code actually covers. Doctors often assume the primary procedure code covers the entire room and everyone in it. It absolutely does not.
The cpt code for ect only pays for the psychiatric service. It pays for your psychiatrist applying the stimulus and monitoring the patient. It does zero to cover the anesthesia. If your billing team tries to wrap the sedation into the main psychiatric claim, the payer will kick it back immediately. Your anesthesiologist must bill their own specific code separately. When you separate the psychiatric professional fee from the anesthesia fee, your denial rate for the cpt code for ect will drop overnight.
Understanding the True Scope of the CPT Code for ECT
If you want to protect your practice’s income, you need to draw a hard line between the different services happening in the treatment room. The core code we are looking at is cpt code 90870.
The AMA defines this simply as electroconvulsive therapy, including necessary monitoring. But as a practice owner or clinic director, you know that simple definitions in medical billing are usually traps. When you bill the cpt code for ect, you are telling the insurance company that a credentialed psychiatrist evaluated the patient immediately prior to the procedure, administered the electrical stimulus, and managed the clinical response.
You cannot survive in this business if your team uses guesswork. You must train your medical coders to view the cpt code for ect as just one single slice of the billing pie.
| Service Component | Covered by the CPT Code for ECT? | Billed Separately? | Responsible Party |
|---|---|---|---|
| Application of electrical stimulus | Yes | No | Attending Psychiatrist |
| Immediate post-seizure monitoring | Yes | No | Attending Psychiatrist |
| Full Evaluation and Management (E/M) | No | Yes (Requires Modifier 25) | Attending Psychiatrist |
| Intravenous general anesthesia | No | Yes (Use CPT 00104) | Anesthesiologist |
| Surgical suite or recovery room fee | No | Yes (Via Revenue Codes) | Hospital or Surgery Center |
| Routine intra-procedure EEG | Yes | No | Attending Psychiatrist |
Look closely at that table. If your front office tries to bundle facility overhead or IV sedation into the cpt code for ect, you will not get paid. Period.
Matching Your Notes to the 90870 CPT Code Description
Auditors do not care about your patient’s feelings; they care about your paperwork. To successfully keep the money you earn, your clinical documentation must flawlessly match the 90870 cpt code description.
Insurance reviewers look for specific, undeniable proof that the treatment happened exactly as billed. First, the provider’s note must document the pre-treatment evaluation. The doctor has to explicitly state the patient is cleared for the procedure on that specific date. Second, the chart needs hard numbers.
You must record the duration of the electrical stimulus. You must record the exact length of the motor seizure. You must record the exact length of the EEG seizure. And you absolutely must specify the electrode placement—whether it was unilateral, bilateral, or bifrontal.
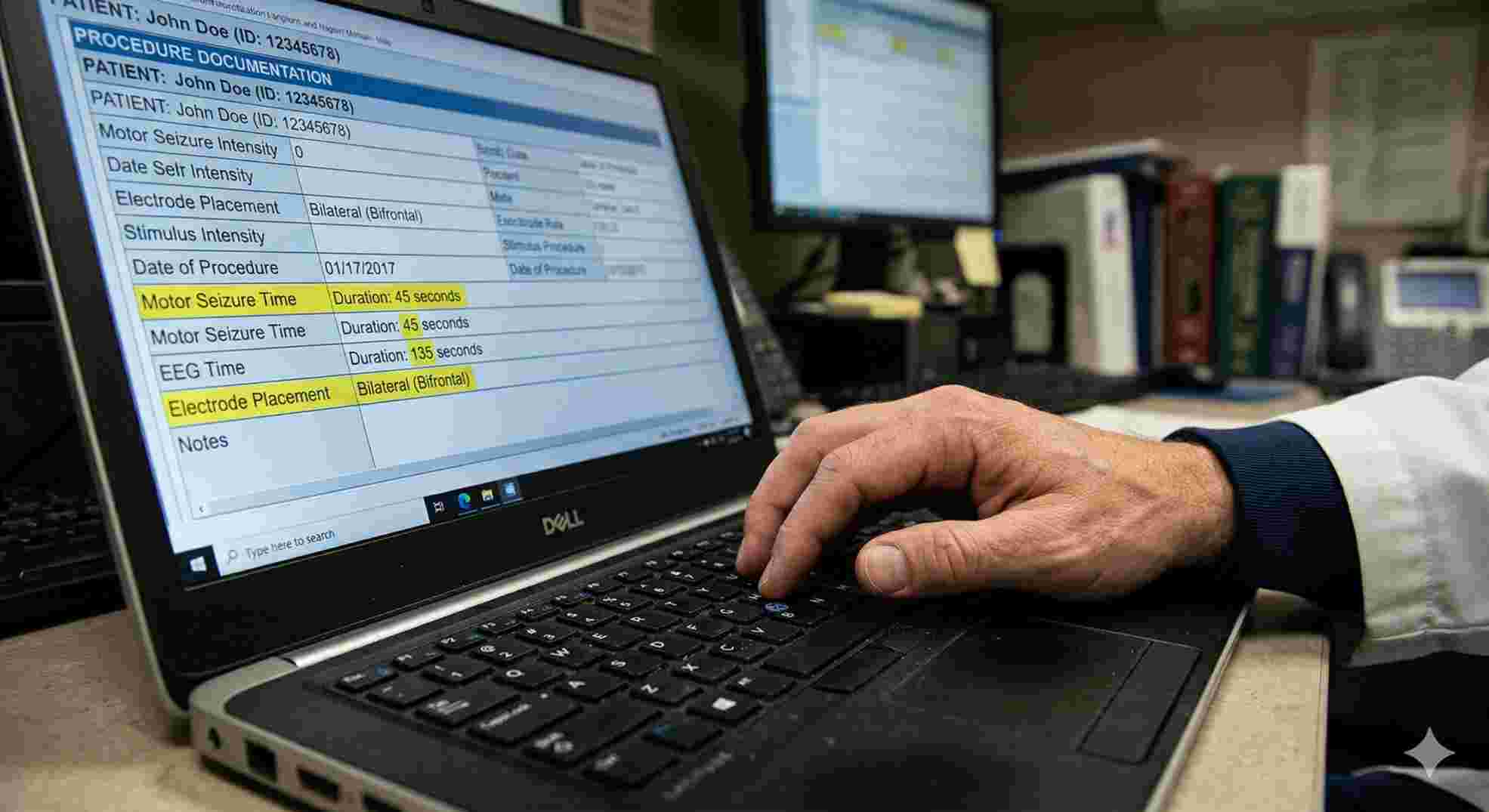
If a Medicare auditor opens your file and just sees a generic note saying “Procedure successful, patient tolerated well,” they will demand their money back. To safely use the cpt code for ect, your charting must be rigorous, numeric, and highly specific. There is no room for lazy documentation.
Medical Necessity in ECT and Mental Health Billing
This is the hardest part of the business. You can code perfectly, but if the insurance company decides the treatment wasn’t medically necessary, they will deny the claim. Because this is an extreme, high-cost intervention, payers will not approve the cpt code for ect for someone dealing with mild, situational sadness.
In the complex world of ect and mental health billing, your ICD-10 diagnosis codes make or break your revenue. The diagnosis has to justify the aggressive nature of the therapy, aligning with the guidelines set by organizations like the American Psychiatric Association.
| ICD-10 Code Group | Clinical Condition | Payer Audit Risk | Documentation Required to Win |
|---|---|---|---|
| F32.x | Major Depressive Disorder (Single Episode) | High | Must clearly document complete failure of multiple psychopharmacology trials. |
| F33.x | Major Depressive Disorder (Recurrent) | Low | Highly accepted, especially if severe or psychotic features are present in the chart. |
| F31.x | Bipolar Disorder | Medium | Must support the presence of severe, unmanageable manic or depressed phases. |
| F20.x | Schizophrenia | Medium | Best supported and quickly approved when the patient exhibits acute catatonia. |
To protect your claims for the cpt code for ect, the patient’s intake history needs to tell a story of treatment resistance. You have to list out the specific antidepressants or antipsychotics the patient took. You must list the dosages. You must explain why they failed.
If the patient is acutely suicidal, or if they have stopped eating and drinking due to severe catatonia, put that in the very first line of the note. When a claims adjuster reviews your submission for the cpt code for ect, they need to see that this therapy was the only safe medical option left.
The Rules for Prior Authorization
You cannot just book a room, treat a patient, and send out a bill. Almost every single commercial health plan, and many Medicare replacement plans, mandate a strict prior authorization before you can even think about billing the cpt code for ect.
When your authorization team calls the insurance company, they usually have to request a specific block of sessions. An acute phase of treatment is typically somewhere between 6 and 12 sessions. You must get the exact dates of service approved.
Then you have to worry about frequency limits. The general industry standard for the cpt code for ect is three sessions per week during the acute phase. If you try to bill four sessions in a single week, the clearinghouse software will likely flag it as a duplicate or an error. If a doctor decides a patient needs a different schedule, or if the patient is stepping down to maintenance therapy once a month, your clinical notes must clearly explain why.
Why Place of Service Matters So Much
Because this treatment requires general anesthesia and induces a medical event, you will almost never bill the cpt code for ect in a standard, outpatient therapy office.
If you put Place of Service (POS) 11 on your CMS-1500 form, you are basically begging the insurance company to audit you for fraud. They know you cannot safely knock a patient out and induce a seizure in a standard office setting without specialized equipment.
The compliant POS codes for the cpt code for ect are highly specific to medical facilities.
| Location / Provider Entity | Specific Service Billed | Billing Form Required | Where the Money Goes |
|---|---|---|---|
| Attending Psychiatrist | CPT 90870 | CMS-1500 | Your practice’s professional revenue. |
| Anesthesiologist | CPT 00104 | CMS-1500 | Directly to the anesthesia group. |
| Hospital / Outpatient Facility | Revenue Code 0901 | UB-04 | To the hospital for the bed and equipment. |
You will normally use POS 21 (Inpatient Hospital) or POS 22 (On-Campus Outpatient Hospital). Sometimes you will see POS 24 if the work happens in a highly specialized Ambulatory Surgical Center.
You have to coordinate with the hospital’s billing department. If you submit your professional claim for the cpt code for ect, but the hospital forgets to submit their facility claim, the insurance company will hold your money. They want to see both claims hit their system so they know the procedure actually happened in a safe environment.
Defeating Denials for the CPT Code Electroconvulsive Therapy
Even when you do everything right, insurance companies will still deny claims. They rely on the fact that most practices will not fight back. As a healthcare business owner, you cannot afford to write off these expensive procedures. You need a system to fight and win.
Breaking Down Specific Payer Rejections
Let’s look at the exact reasons your claims fail and how to build an operational defense against them.
The Missing Modifier Denial
Sometimes a psychiatrist will evaluate a patient in the morning, decide they need treatment, and then perform the procedure that afternoon. If your team bills a standard Evaluation and Management code (like 99222) alongside the cpt code for ect on the same day without a modifier, the payer will deny the E/M code. They will say the evaluation was already included in the surgical package.
How to Win the Modifier Appeal
You have to use Modifier 25. Append Modifier 25 to the E/M code. This tells the insurance company that the morning evaluation was completely separate and significant from the actual procedure.
A Quick Note on Charting Requirements
Make sure your doctor wrote two distinct, separate clinical notes for the evaluation and the procedure. Do not mix them on the same page.
The Medical Necessity Denial
This is the one that makes doctors furious. A payer algorithm looks at your submission for the cpt code for ect and decides the patient didn’t really need it.
Fighting Back with Clinical Facts
Do not just resubmit the claim. You must write a customized appeal letter. Pull the patient’s entire medication history. Highlight the failed drug trials. Quote the insurance company’s own medical policy back to them, showing exactly how your patient meets their criteria for the cpt code electroconvulsive therapy.
The Date Mismatch Error
This is an incredibly common administrative error. Your practice bills the cpt code for ect for a Tuesday. The anesthesia group accidentally bills their code for Wednesday. The insurance company’s software sees a psychiatric procedure with no anesthesia, and an anesthesia bill with no surgery. They deny both immediately.
Building an Internal Hard Stop
You need a hard stop in your billing process. Before any batch of claims leaves your office, a biller must manually verify that your dates of service, patient names, and diagnosis codes perfectly match what the facility and the anesthesiologist are submitting.
Streamlining Your Internal Revenue Operations
You cannot grow a behavioral health business if you treat complex medical billing like casual data entry. Submitting the cpt code for ect requires a dedicated, specialized workflow.
Assign one specific person in your front office to handle all prior authorizations for these procedures. The clinical requirements are incredibly strict. Having one specialist who knows exactly what the major payers want to hear will drastically cut down your waiting time for approvals.

Next, you need to audit your own doctors. Every month, pull five random charts where you billed the cpt code for ect. Read the notes. Are the doctors documenting the exact seizure times? Are they clearly stating the electrode placement? If they are using a basic copy-and-paste template that says the same thing for every patient, make them stop today. Official federal reviewers at Medicare use sophisticated software to catch cloned notes, and they will demand massive refunds if they catch you doing it.
Final Thoughts on Protecting Your Claims
Stop accepting claim denials as just a normal part of doing business. You are providing a life-saving medical service, and you deserve to be compensated accurately and quickly. By respecting the strict boundaries of the procedure, demanding exact clinical details from your providers, and fighting back against unfair payer rejections, you can take total control of your revenue cycle. Ensure your documentation is flawless, master your modifiers, and build a system that confidently submits the cpt code for ect correctly the very first time.